+91 9650760803
+91 9650760803 

Interstitial Pulmonary Fibrosis
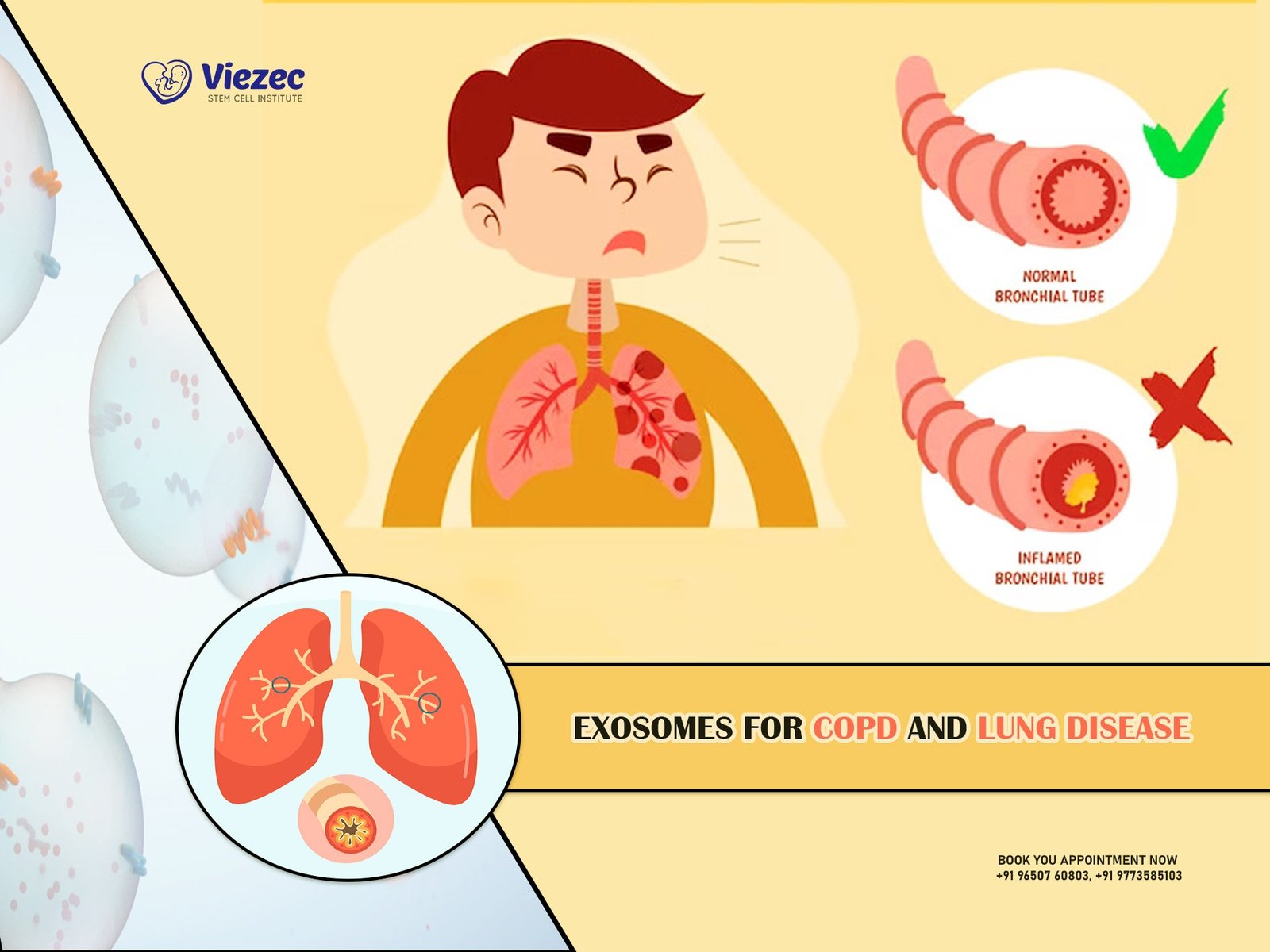
Interstitial lung disease (ILD) and diffuse parenchymal lung disease (DPLD) are lung illnesses that damage the tissue and spaces surrounding the air sacs (interstitium) in the lungs (alveoli). This group of lung diseases is caused by an injury to the lungs that does not heal correctly for a variety of causes. The following parts of the lungs are vulnerable to injury:
- Pulmonary capillary endothelium
- Basement membrane – a specialised kind of extracellular matrix (ECM)
- Alveolar epithelium – a functional and physical barrier to harmful environmental chemicals
- Perivascular tissue • Perilymphatic lung tissue
Pulmonary Fibrosis Signs and Symptoms
The following are some of the most frequent signs and symptoms seen in individuals with onset idiopathic pulmonary fibrosis:
- Excessive gasping for air. This is caused by heart disease or by the body receiving less oxygen as a result of inefficient, damaged alveoli. Physical exercise makes it worse since the body is attempting to obtain more oxygen.
- Dry cough that persists.
- Feelings of clubbing in the fingers and toes. The swelling at the base of the finger is known as clubbing, and it is often accompanied by cyanosis (bluish discoloration of the nails.) This is an indication of hypoxia, or a lack of oxygen in the tissue. This symptom usually appears as the illness progresses and the patient reaches end-stage pulmonary fibrosis.
- Premature tiredness due to a reduction in lung capacity or airflow blockages
ILD & IPF Lung Scarring
Patients frequently question how they acquire fibrotic scarring of the lungs since the underlying cause of idiopathic lung fibrosis is often unclear. The following are the most frequent risk factors for developing interstitial lung disease and alveolar fibrosis in most patients:
- Interstitial pulmonary fibrosis is often caused by cigarette smoking.
- Genetic – Familial fibrotic scarring of the lungs;
- Reaction to medicines or treatments such as antibiotics, chemotherapy drugs, and cardiac dysrhythmia therapies (antiarrhythmic);
- Inorganic poisons, chemicals, and pollutants such as asbestos, beryllium (berylliosis), and crystalline silica dust (silicosis)
- Organic substances, dust, fungus, or mould exposure (hypersensitivity pneumonitis)
Pneumocystis pneumonia (PCP), TB, atypical pneumonia, chlamydia trachomatis, and syncytial virus are examples of viral illnesses.
- Gastrointestinal reflux disease (GERD) (Gastroesophageal reflux disease). This occurs when a patient’s stomach contents return to the oesophagus. There is a chance that these stomach contents may be aspirated into the trachea, causing a lung infection.
- Lupus, rheumatoid arthritis, polymyositis, dermatomyositis, lymphangitic carcinomatosis, antisynthetase syndrome (inflammation), and systemic sclerosis
- Inflammatory bowel disorders such as ulcerative colitis and Crohn’s disease
- Antisynthetase syndrome (inflammation) and systemic sclerosis
The administration of mesenchymal or hematopoietic stem cells through intravenous, organ-directed, or nebulizer routes is known as stem cell therapy. In the case of COPD stem cell treatment, stem cells may help to heal lung tissue damage by regenerating tissues and secreting cytokines. Aside from their ability to repair and rejuvenate, stem cells have inherent immunomodulatory characteristics that may aid the body in fighting cytokine storms. According to research studies, COPD stem cell therapy has improved patients’ oxygen retention capacity and reduced breathing problems. Aside from traditional medications and breathing assistance, stem cell therapy for lung disorders has emerged as the most effective treatment option. Although stem cell treatment is currently an experimental approach that can not cure severe lung diseases, it has proved to be the most effective way to get good outcomes. Given the existing treatment procedures, which need ventilators and complete lung transplants, which are both uncommon and costly, stem cell therapy is becoming more popular.